When I was pregnant for the first time, I was focused completely on making sure that our son was born safely.
I thought that I need to concentrate my energy on giving birth – and the rest will be a piece of cake.
Today I know how wrong I was because AFTER giving birth is when it REALLY starts. 😉
All the check-ups, shots, breastfeeding, postpartum issues, sleepless nights… Let me tell you, it’s a lot! With our second baby it was easier, but on top of the usual bitter-sweet madness 😉 it turned out that our daughter had problems with her hips. As early as two days after her birth, we were told to take a closer look at them.
WHAT CAN BE WRONG WITH YOUR BABY’S HIPS?
The socket and bones that build a baby’s hip joints are delicate and can easily disconnect from each other. They mature over time to make the hip joint stable.
To put it very simply, the hip joint consists of two elements: the (1) ball of the thighbone, which should be located centrally inside the (2) socket. These two elements are rather loose, but over time they grown into to each other so that they become practically inseparable. 😉
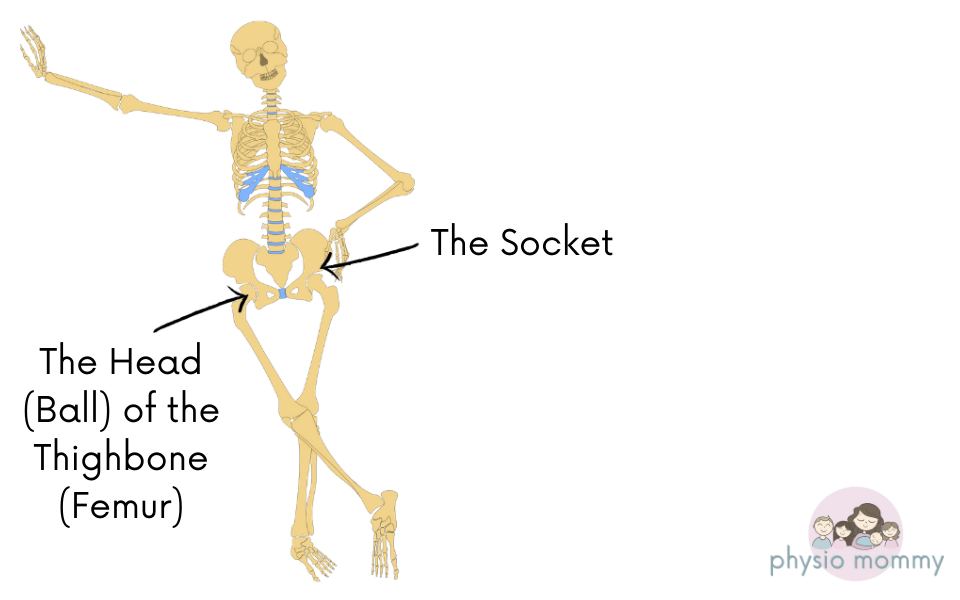
When a baby is small, these structures are delicate and not yet fully formed. It can happen that the ball, instead of “sitting” quietly in the socket and shaping it, decides to “explore” the area. This happens especially when the socket is shallow or has steep edges – then each time the head (the ball) is pushed out of it, it can damage the hip joint.
In extreme cases, the head of the femur does not return to its place, – which means dislocation of the hip – which fortunately is rare.
WHAT IS THE DIFFERENCE BETWEEN DYSPLASIA AND NORMAL IMMATURITY OF THE HIPS?
To put it simply, hip dysplasia happens when the head of the thighbone shifts to the side and permanently slides out of the socket of the hip joint.
Normal physiological immaturity means that the relationship between the head of the thighbone and the socket is still maturing. 😉
WHAT ARE THE RISK FACTORS OF DYSPLASIA?
- Hip dysplasia affects girls more often than boys (that was the case with my children). 😉 It is because the hormone relaxin, which plays an important role during pregnancy and labor by relaxing the joints, still has an effect on baby girls. 😊 Dysplasia in girls happens six to eight times more often than in boys.
- Dysplasia develops more often in children from first pregnancies, in children who have a family history of dysplasia, in children with a large body weight.
- Risk factors also include twin or multiple pregnancies, low levels of amniotic fluid, premature birth, and breech positioning of the baby.
Oddly, the problem concerns the left hip, much more often because of the position of the baby in the womb. In the vast majority of cases, babies are positioned with their left hip against the mother’s spine, which limits the movement of the left leg. It is in the bent position that the elements of the hip joint fit together best. 😊
If your child is at risk or the doctor finds some abnormalities, you will be referred to a specialist for an exam and probably an ultrasound around 6 weeks of age. Such an examination shows how the individual elements of the hip joint are positioned in relation to each other.
WHAT DOES THE EXAMINATION LOOK LIKE?
When examining the hip joints, the doctor pays attention to the activity of the legs, their length, the skin creases (although uneven skin creases do not necessarily indicate the existence of dysplasia), checks the range of motion in the hip joints, and also performs special tests in order to assess how easily the head of the thighbone comes out of the socket.
If the doctor checks by ultrasound, the baby will be placed on the side and you will be asked to hold his or her legs. The doctor will put some gel on the hip area and run the camera head over the area in order to take the necessary measurements
After the examination, the doctor will recommend a follow-up visit or appropriate treatment.
WHAT SHOULD RAISE A RED FLAG?
Although detection of irregularities in the hip joints is quite efficient, it is still worth observing your baby. In case of any doubts, inform your pediatrician about your concerns.
You should be concerned when you notice a clear disproportion in the movement of the legs, when one of the legs seems to be shorter than the other, when the skin folds on the buttocks or thighs are asymmetrical. Also, if you hear or feel clicking in one of the hips (the majority of clicking sounds should spontaneously disappear around the second week of life) or when one of the legs has a limited range of movement.
It is worth remembering that some children develop dysplasia in both hips, so capturing asymmetry in their structure or movement may not be so easy. If that’s the case, the above mentioned medical exam or an ultrasound will be helpful.
WHAT DOES PREVENTION LOOK LIKE?
This is my favorite part. 😊
I believe that if the hips require treatment, there is no point in looking for solutions on your own, but use orthopedic equipment recommended by the doctor.
If it’s a case of normal physiological immaturity, we leave the hips as they are which basically means nothing more than:
– making sure the hips have maximum freedom of movement (don’t use onesies and tight sleepers, don’t pin diapers too tightly);
– providing a variety of experiences; avoiding soft mattresses, bouncers, and keeping the baby in a semi-reclined position on the back – all which limit movement.
– putting the baby on the tummy BUT WITHOUT PRESSING DOWN HIS OR HER BUM!
– avoiding movements that could provoke the head of the thighbone to slide out of the hip socket. 😊 What does it mean? When changing diapers, don’t pull the baby by the legs, but lift his or her bum or use elements of rotation and baby-friendly care. Avoid situations in which the baby’s legs are together or the feet are far apart. Also, do not wrap the baby in a baby blanket where the legs are straight.
– carrying your baby facing you, but with legs spread out and bum resting over your forearm. If your little one starts to fuss and arch his back, you can sit with your baby in this position, but at an angle to the floor. 😊

WHAT ABOUT BABY WRAPS?
The position of a baby’s legs in a wrap is actually similar to the one used in the treatment of hip dysplasia.
However, you have to bear in mind that carrying your baby in a baby wrap should not replace proper treatment if the hips require it.
There is also one condition – the wrap should be tied well. I encourage you to find out how to tie your wrap with the help of a specialist who can easily see if wrapping needs correction.
It is important to remember that the position of the child’s legs in the wrap is not without significance. First of all, they should be bent so that the knees are below the child’s navel. However, they should not be spread out too much (in the youngest babies up to 60 degrees). When the hips are too far apart it can contribute to insufficient blood flow to the head of the thighbone, which of course, we do not want to happen. The feet should be facing outward.
DOUBLE DIAPERING
While this is a widely recommended practice, it is not really justifiable for several reasons.
First of all, in case of hip dysplasia, first and foremost you should focus on using suggested orthopedic equipment. Double diapering, is not a guarantee of success since there is no control over the whole process (the diaper can move and slide).
When we are dealing with physiological immaturity of the hips double diapering or any other special exercises are not needed.
In addition, carrying around several layers of diapers is not without impact on the position of the baby’s pelvis, which in turn can affect the overall activity of the baby.
SOMETHING OPTIMISTIC AT THE END
I know that many parents whose children need treatment worry about their further development. It’s understandable since their children work in completely different conditions than babies whose hips are developing properly.
However, keep in mind that at the moment, the hips should be your priority. And probably, you are going to forget about the whole treatment sooner than you think.
In a study that evaluated the effect of hip dysplasia treatment on child development (the average duration of treatment was 13 weeks), it was shown that these babies began to sit at 7 months of age (a week later than children from the control group) and walk at 12 months and 2 weeks (3 weeks later than children from the control group). As you can see it’s not a significant difference. 😊
From my own experience, I can add that really, the vast majority of children quickly catch up with their peers. (Phew – thank God for natural drive for development! 😉). However, sometimes it doesn’t hurt to ask a specialist for guidance. So, if you have a baby whose hips require treatment, keep calm and deal with the problem. In case of any doubts, go see your pediatrician or a pediatric physical therapist. Your child will certainly surprise you more than once! 😊
Have you made it to the end? 😉
Every day you influence your baby’s life by the things that you do. Check out my ideas for fun and smart playtime activities to help your baby’s development!
Sources:
- Kotlarsky, P.; Haber, R.; Bialik, V.; Eidelman, M. (2015), “Developmental Dysplasia of the Hip: What Has Changed in the Last 20 Years?;” World Journal of Orthopedics, vol. 6 (11), pgs. 886–901.
- “THE FIRST 2 YEARS OF A CHILD’S LIFE;” Medycyna Praktyczna, Krakow 2012
- Consent, M; Wasilewski, P; Wasilewska; Golicki, D (2010), “Influence of the Treatment of Developmental Dysplasia of the Hip by the Abduction Brace on Locomotor Development in Children;” Journal of Children Orthopaedics, Feb 2010; vol. 4(1), pgs. 9–12.
- AMERICAN ACADEMY OF PEDIATRICS (2000), Clinical Practice Guideline: Early Detection of Developmental Dysplasia of the Hip; Pediatrics, April 2000, vol. 105 (4), pgs. 896-905.